
The journey to accessibility excellence
Here at CURE Niger, as with all CURE hospitals throughout the network, we’re striving to serve the children of our country who are needlessly suffering from treatable disabilities—like clubfoot, bowlegs, neglected broken bones, and burn contractures, to name just a few.
With our intense focus on treating children, getting them walking for the first time or allowing them to use their hands again, though, we’ve developed a blind spot. Unfortunately, we’ve glossed over many of their other needs before they’re fully healed and have missed chances to make them more comfortable and at home in our hospital—both when they first arrive and as they stay with us during their recovery.
Accessibility is not really a thing in Niger, and construction is definitely not designed with those among us with special needs in mind. You’ll be hard pressed to find a wheelchair ramp in our country, and in my years here, I have yet to see handicap-accessible parking spaces. While this is the reality in Niger, it does not give us at CURE Niger permission to also fail at providing accommodations to those with special needs because 1) this is exactly who we are here to serve and 2) we strive to operate at the highest standards even if they exceed what is required by local regulations.

Realising we were lacking in this area was half the battle. We struggled to move forward as, frankly, we don’t know what we don’t know. To help us get our hospital to the point where it is accessible to all, we enlisted the help of our long-time partner CBM to conduct an Accessibility Audit on both our facilities and our operations. If you don’t already know, CBM is an international Christian development organisation with a goal to improve the quality of life for persons with disability in some of the poorest countries of the world. They advocate for the rights and dignity of people with disabilities and strive to create inclusive spaces where people with disabilities are known for what they can do as opposed to what they cannot. CBM points out that “accessibility is a prerequisite for inclusion,” as without accessible construction and institutions, people with disabilities cannot access services, information, and resources, rendering full inclusion impossible.
Knowing our shortcomings in the area of accessibility, we not only saw an opportunity to improve by partnering with CBM but also an opportunity to begin a larger, country-wide conversation about accessibility. Rather than just have CBM come in and conduct an accessibility audit on our hospital, we hosted a week-long training session where representatives from all over Niger attended, learned about the various needs of different disabilities, discussed what is meant by “reasonable accommodation” and “universal design principles,” and practiced how to conduct an accessibility audit, spot issues, and recommend ways an institution can improve both its accessibility and inclusion for those with disabilities. The idea behind all this is that the attendees with then be able to return to their home institutions with this training and slowly shift Nigerien culture to be a more accommodating and inclusive culture!
Now before we go patting ourselves on the back for hosting this training and hopefully being part of a more inclusive future, neither the auditors nor the trainees went easy on us. The audit came back and we have a lot of work to do.

As you might guess, we have a lot of patients in wheelchairs. We don’t have too many that show up in wheelchairs—most can’t afford one or don’t need one before surgery—but once they receive surgery, sometimes having both legs in casts simultaneously, they’re wheelchair-bound for a minimum of six weeks, if not a full three months.
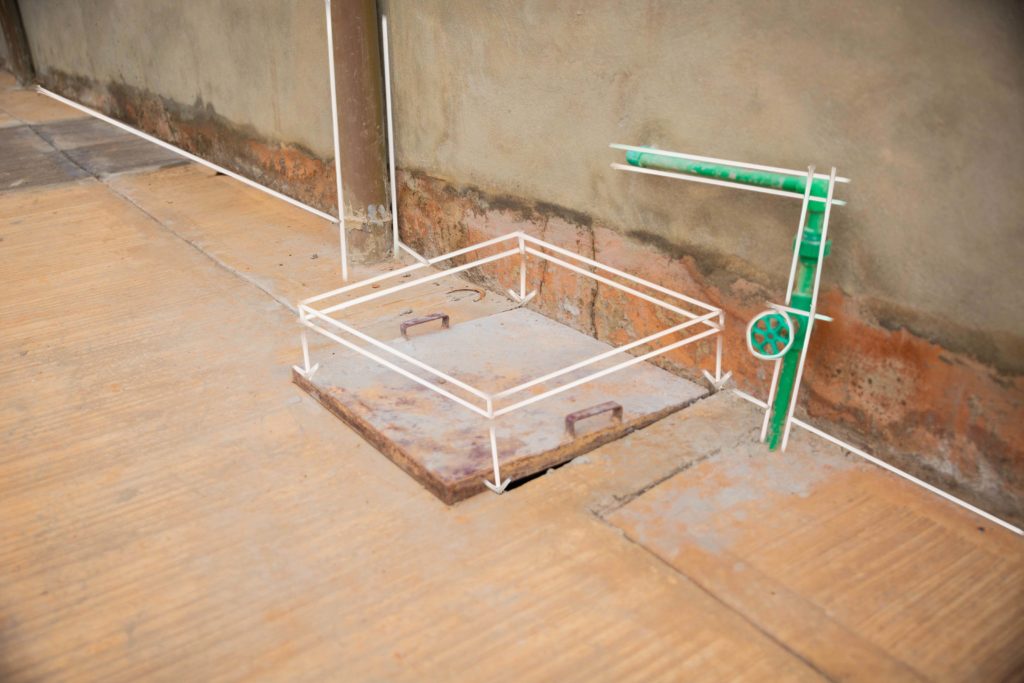
This was true for a patient called Gail, who was wheelchair bound for a significant portion of 2018 after receiving multiple surgeries for her severely bowed legs. Staff and patients came around Gail to support her and assist her during her time in a wheelchair, but the CBM Accessibility Audit pointed out a number of areas where we could improve to have allowed Gail more independence during her recovery. We could have (and should have) expanded our sidewalk and road paving instead of relying on hard packed dirt as is normal in Niger (only about 20% of the roads here in the capital city are paved). The audit also pointed out many of the paved areas we do have tend to be cluttered, are not wide enough for a wheelchair to turn 180 degrees, and have ill-fitting manhole covers. Along these same lines, the audit noted that while we do have wheelchair ramps to all our buildings, all but one of their slopes are too steep for a person in a wheelchair to easily access the building without help. Another area we didn’t consider was the height at which we layed out our buildings. The audit pointed out that our service counters, door handles, window latches, light switches, and fan controls are all far too high to be accessible, requiring someone in a wheelchair to ask for help in order to reach them.

Due to the nature of open fire cooking and the heavy use of cooking oil in Niger, a large number of our patients come to us with old burns that have healed in a way that make their fingers unusable. Jamila, who burned her hands when she tripped and fell, plunging her hands into a pot of boiling cooking oil, is a perfect example. As she healed from her burns, she did so in a way where all her fingers were essentially melted together. While her finger bones and muscles were still there, her skin stretched over them like mittens make using her individual fingers useless to her. The audit pointed out that for patients like Jamila, both our doors and our windows were unusable. High accessibility standards, like the ones we are striving for, state that doors and windows should be able to be locked, unlocked, opened, and closed by using a closed fist in order to be accessible. While we are working to release Jamila’s fingers, changing our door handles and window latches is just one small change we could make to give her and patients like her more independence and foster a more inclusive space for them.
Finally, the CBM audit looked at our institutional accessibility. The looked at the ideology behind our methodology, how we use our words and messaging to let people with disabilities know they are welcome to be a part of what we do. The audit brought to our attention we don’t have any clauses to disability inclusion and we currently do not have any employees with disabilities. We need to make it clear that qualified people with disabilities are welcome to apply for any of our open positions and we have the facilities to accommodate special needs. As a side note, while CURE Niger has some work to do in this area, other CURE hospitals around the network are further along this journey towards excellence than we are. For inspiration, we can look to hospitals like CURE Zambia and their on-site partnership with the Zambian Association for Children with Disabilities and CURE Kenya, where one of the most beloved employees is Peter, whose hearing loss does not stop him from ministering to children and engaging in the mission of CURE.
Some of these issues we have known, but many we did not. Already before the audit, we’ve been working on expanding our network of paved sidewalks and roads. For the first time in our nine years as a hospital, our patient guesthouses are now connected to the rest of the hospital by wide, level, and uncluttered sidewalks, allowing patients to easily attended their regular bandage changes and doctors appointments. We’ve also started installing railings around our raised sidewalks and have been altering our wheelchair ramps to make them more independently accessible.
There’s a lot of work to be done and, in all honesty, once we have carried out all of the audit’s recommendations, there will still be work to be done. Inclusion is not a destination but an ongoing conversation about how we can best serve our patients and the population with disabilities here in Niger. Our mission is to decrease this population through treatment while also building up our infrastructure and institutional practices in a way that allows them access to the resources and independence we all crave.
Learn more about our commitment to essential surgery at cure.org/uhc
Footnote: Article written by Joel Witwer on Tuesday 24th September 2019